Emergency medicine has always demanded more than clinical knowledge. It demands quick decision making with high precision — in the room, under pressure, when stakes are at their highest. In January 2026, ABEM made measuring that official. The oral certification exam updated to a hybrid assessment that now formally tests communication skills, professionalism, procedural competency, and clinical reasoning in live, standardized patient encounters.
For EM residency programs, this is not simply a format update. It is a refinement of what the specialty considers a competent physician.
Most board prep resources available to residents were built for the exam that no longer exists. What residents need now is a resource built around how the new exam actually tests across clinical reasoning, communication, and clinical skills.
What actually changed in the 2026 ABEM certifying exam?
The 2026 certifying exam replaces the traditional oral boards with a hybrid format built around two distinct case types, administered in person at the AIME Assessment Center in Raleigh, NC. Here is what changed:
%25201.png)
Source: ABEM certifying exam overview
The most significant change is in focus. The oral exam tested one thing: clinical reasoning. The 2026 certifying exam tests four — reasoning, communication, professionalism, and procedural competency — assessed in live, standardized patient encounters that the previous format never included. Everything else, the move to in-person, the shorter station format, the nine exam windows per year, follows from that fundamental expansion of what the specialty now formally defines as competency.
Why does traditional board prep fall short for the new ABEM exam?
The board prep infrastructure most programs use — review courses, question banks, oral case books — was designed for an exam that is no longer current.
Question banks develop knowledge recall. They are useful for the written qualifying exam and remain part of the preparation picture. But they do not provide adequate clinical context for higher order thinking. Oral case books were built for the old oral board format — a reasoning discussion, not a performance assessment. They do not include standardized patients, they do not score communication, and they do not simulate procedural competency in a live interaction.
Building in-house case preparation addresses the gap, but it is time consuming, expensive and operationally demanding. A properly functioning standardized patient program requires trained SPs, dedicated exam rooms, faculty calibration, and ongoing QA infrastructure. Most programs do not have that capacity at the scale needed to prepare an entire cohort, across nine exam windows, year-round.
The practical result: residents are being asked to prepare for a performance-based exam with tools built for a knowledge-based one.
How can EM residency programs prepare residents for a performance-based exam?
Addressing the gap requires repeated, realistic encounter practice — not more case review. Residents need to perform in simulated patient interactions enough times that the communication skills, reasoning process, and procedural sequencing become consolidated.
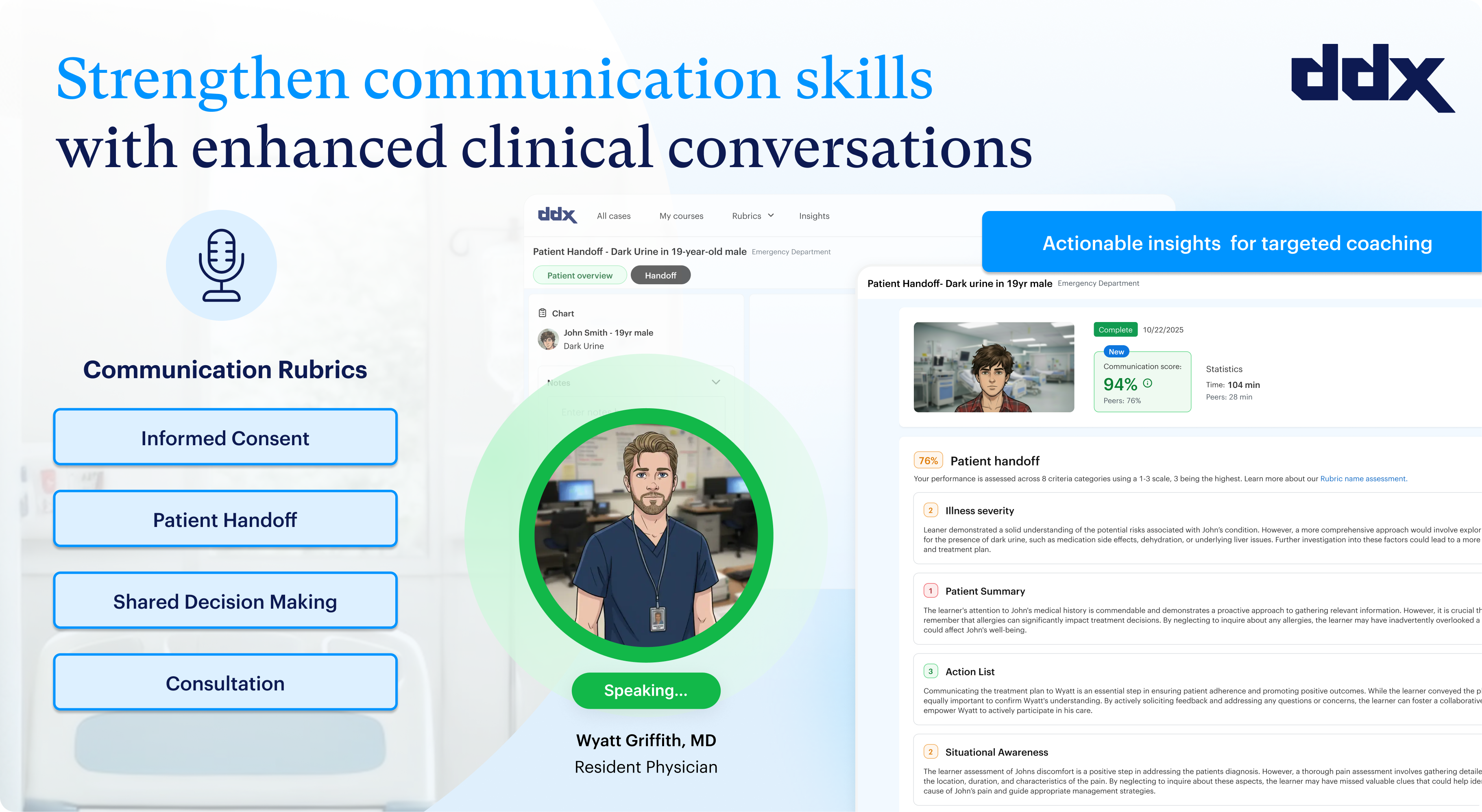
DDx by Sketchy is built for exactly this kind of preparation. The platform delivers AI-enabled patient simulation across clinical reasoning, communication, and clinical skills — the three competency categories the recently updated ABEM exam now formally tests.
Residents can work through realistic, multi-role encounters repeatedly, at their own pace, without requiring trained SPs, room setup, or manual faculty scoring. Automated rubric-based feedback gives residents immediate insight into where their communication or reasoning broke down, and program directors get cohort-level data to identify gaps before exam windows open.
Critically, DDx scales. Programs can deploy it continuously across a full resident cohort — not just for a pre-exam sprint, but as ongoing clinical readiness infrastructure throughout the year.
See how EM programs use DDx for year-round clinical readiness
The 2026 ABEM certifying exam tests across three distinct competency domains — clinical reasoning, communication, and procedural skills. DDx is built around the same structure.
Rather than a single simulation format, the platform gives programs the flexibility to deploy targeted cases by competency and stage of training, mirroring how clinical readiness actually develops across a residency year. Programs can assign:
- Clinical reasoning cases that build task prioritization across multiple patients — helping residents develop a sense of sick vs not-sick on a busy patient board.
- Clinical skills cases that develop fluency in high-yield presentations, reinforcing adaptive reasoning as patient data evolves: labs, imaging, treatment response, and clinical status.
- Communication cases that give residents structured practice in handoffs, consults, escalations, and difficult clinical conversations — the same skills ABEM now formally scores.
The result is a board prep strategy that isn't front-loaded into a pre-exam sprint. Programs can build clinical mastery continuously across training years.
Try DDx free at educators.sketchy.com to see how it fits your program's preparation strategy.
Frequently asked questions
What changed in the 2026 ABEM certifying exam?
The 2026 ABEM certifying exam replaced the traditional oral boards with a hybrid format that tests four competency domains: clinical reasoning, communication, professionalism, and procedural competency. These are assessed through live, standardized patient encounters administered in person at the AIME Assessment Center. The previous oral format tested clinical reasoning only, through a case discussion rather than a live performance assessment.
What does an effective ABEM board prep program look like for EM residencies?
Effective preparation requires repeated, realistic encounter practice across all three competency domains the exam tests: clinical reasoning, communication, and procedural skills. Programs need scalable tools that allow residents to practice asynchronously across the year without requiring trained standardized patients, dedicated room setup, or manual faculty scoring for every encounter.
How does AI simulation support emergency medicine board preparation?
AI-enabled simulation platforms allow residents to work through realistic multi-role patient encounters repeatedly, at their own pace, with immediate rubric-based feedback on communication and reasoning. Program directors gain cohort-level data to identify gaps before exam windows open. This makes structured, performance-based preparation scalable across a full resident cohort throughout the training year.