Residency program directors (PDs) typically know exactly what clinical skills incoming interns need on day one. According to the American Medical Association, 94% of PDs expect residents to gather a history and perform a physical without supervision. 87% expect a coherent oral summary. 77% expect accurate clinical documentation. And yet similar gaps show up every July 1, in the same skills, across programs of every type and specialty.
The way residency programs build these skills is fundamentally misaligned with what residency actually demands. This is a preparation problem and closing that gap requires a structural solution, not just a better orientation week.
In this piece, we examine why the gap persists, which skills PDs are most commonly seeing on arrival, and what a preparation infrastructure that actually closes it looks like.
The five clinical skills: what residency program directors are seeing on arrival
These are the specific skills PDs identified as both most essential and most commonly deficient on arrival (AMA), activities every entering resident should be able to perform without direct supervision, regardless of specialty.
- Gathering a history and performing a physical examination (94%): When underdeveloped, supervision slows, assessments become inaccurate, and problems cascade downstream through oral presentation and documentation.
- Providing an oral presentation of a clinical encounter (87%): When it breaks down, the care team loses a shared understanding of the patient, slowing clinical decisions and increasing the supervisory burden on attending physicians.
- Documenting a clinical encounter in the patient record (77%): Documentation failures on arrival are reasoning and synthesis problems. An intern who can't organize their clinical thinking verbally can't organize it in a note either.
- Participating as a contributing member of an interprofessional team (58%): When underdeveloped, interns become a source of friction rather than function within the care team.
- Recognizing urgency and initiating evaluation and management (51%): Rare enough in UME that many learners arrive without reliable exposure, consequential enough that a gap here carries direct patient safety implications.
The thread connecting all five: they are not knowledge gaps that can be closed with additional curriculum content. They are performance gaps that require a fundamentally different kind of preparation.
Why the intern readiness gap persists in GME
Two compounding factors explain why this gap is predictable rather than random.
Uneven case exposure
PDs inherit variance they had no hand in creating. Two interns from the same medical school can arrive on July 1 with dramatically different clinical experiences:
- Different patient volumes and case complexity
- Different levels of faculty supervision
- No standardized floor for clinical exposure before arrival
Research published in AEM Education and Training found that PDs face genuine uncertainty about the entering skill level of interns, with some not meeting ACGME Level 1 milestones on arrival, creating unpredictability around how to engage new interns at the appropriate level from day one.
The skills themselves resist traditional assessment
The skills PDs flag most often share a common trait: they are performance skills, not knowledge skills. They require:
- Repeated practice against realistic clinical scenarios
- Structured, consistent feedback
- Rubric-based assessment applied longitudinally over time
Direct observation and deliberate practice of these activities in the clinical setting faces real constraints. The curriculum has defined what these skills look like. It has not reliably built the infrastructure to develop them.
How to close the residency readiness gap: what a structural solution requires
The solution to a structural problem is a performance-based infrastructure — one that builds and assesses these specific skills longitudinally, with consistent rubrics, realistic clinical fidelity, and data that follows residents throughout their training.
DDx by Sketchy was designed to deliver exactly that.
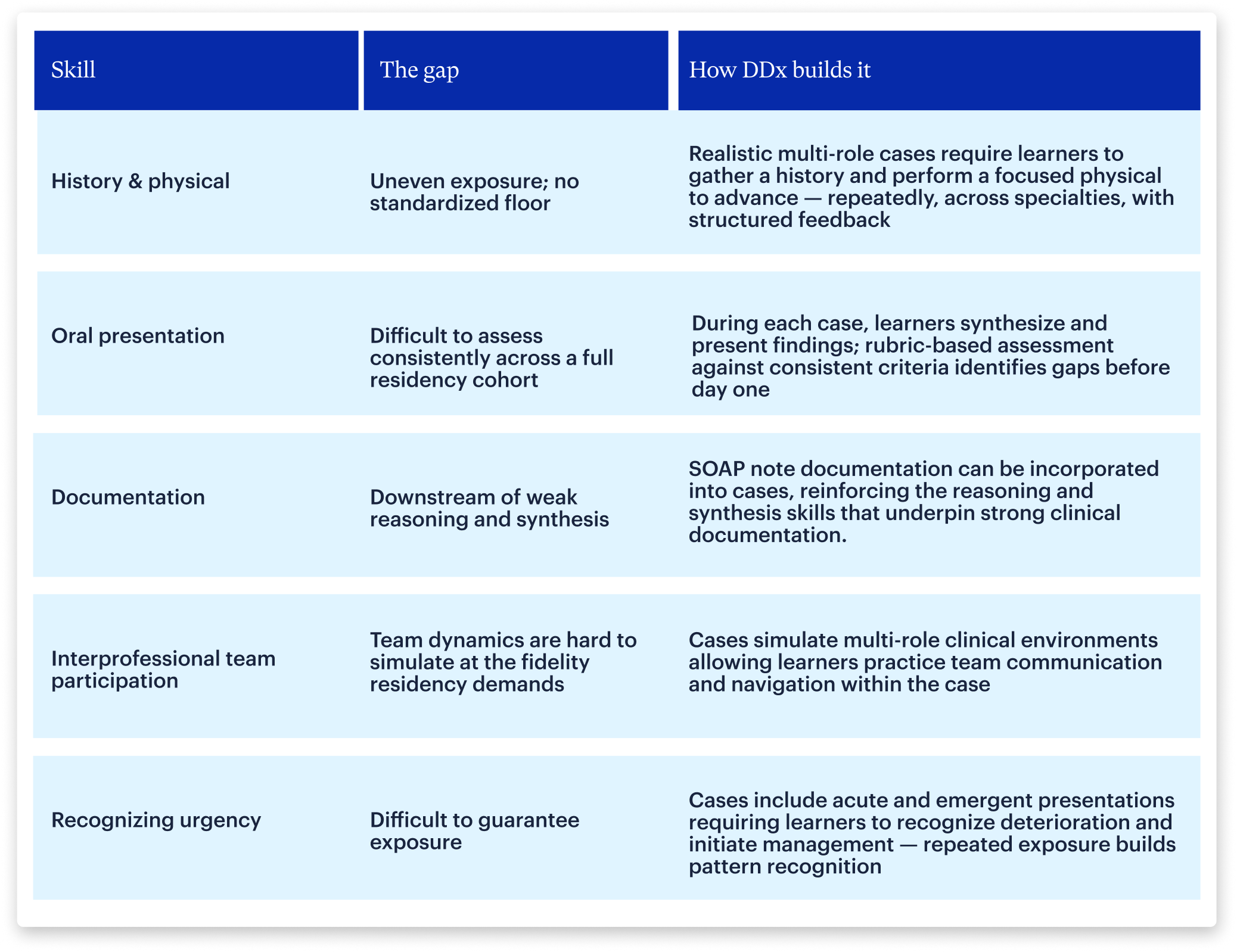
Across all five, DDx delivers what the field's existing infrastructure has not: realistic, multi-role case simulation across every clinical competency, with rubric-based assessment and longitudinal data that gives programs visibility into where learners actually stand before day one.
Build clinical readiness into residency training
Closing this gap requires building readiness into the curriculum and maintaining longitudinal visibility into how residents think, develop, and perform throughout training. For programs ready to act on that question, three things are required:
- Structured, simulation-based preparation that establishes a baseline from day one
- Consistent rubric-based assessment applied longitudinally
- Longitudinal performance data that makes clinical reasoning visible throughout residency
The field has defined what readiness looks like. What remains is the harder question: whether the current curriculum reliably builds those skills or simply assumes they will arrive.