Every accredited Nurse Practitioner program is held to the same outcome standard, but not the same assessment infrastructure.
Organizations like CCNE and ACEN define what graduates must be able to do before entering practice. What they don't define is how programs should evaluate the thinking that leads to those decisions. A 2022 scoping review of U.S. primary care NP programs found "a lack of shared conceptualizations of diagnostic reasoning" across the field — meaning most programs rely on tools that measure what students produce rather than how they think.
That gap looks different depending on how a program is structured:
- Online and hybrid programs struggle with visibility — faculty rarely observe reasoning in real time
- Large-scale programs struggle with consistency — shared evaluation standards break down across dozens of sites and preceptors
- Smaller cohort programs face recognition challenges — from securing clinical placements to attracting the resources students need to succeed
Across all three, the underlying challenge is the same. What differs is not faculty intent or quality — it's what each program structure actually allows faculty to see.
Why do online and hybrid NP programs struggle to assess clinical reasoning?
Online and hybrid NP programs face a structural visibility problem: faculty rarely directly observe students during clinical encounters, and competency evaluation depends heavily on information reported after the fact — typically through online skills submissions or onsite clinical intensives and workshops. Because direct observation is limited to these structured touchpoints, what faculty see is a snapshot, not the full picture of how a student thinks in practice.
Challenges:
- Clinical reasoning is inferred rather than directly observed
- It becomes difficult to distinguish mastery from memorization
- Faculty may struggle to distinguish thinking errors from limited clinical exposure, and addressing either requires time programs can rarely spare
When reasoning gaps go undetected early, they often surface later during higher-stakes evaluations, when remediation becomes more disruptive for both students and programs.
How does scale create inconsistency in large NP program assessment?
Large-enrollment programs face a different structural challenge: when hundreds of students are placed across dozens of clinical sites, maintaining a shared understanding of what strong clinical reasoning looks like becomes a coordination problem that grows with every new cohort.
Challenges:
- Interpretive variance: Different preceptors may define "competent reasoning" differently.
- Limited preceptor capacity: With constrained preceptor resources, programs often lack consistent visibility into how clinical standards are applied across placements.
- Documentation risk: Subjective evaluations can be difficult to standardize, audit, and defend under regulatory scrutiny.
Even well-designed programs struggle to ensure that reasoning standards are applied consistently across sites. The result is a difficult reality for program directors: they remain accountable for outcomes they cannot fully observe or verify.
Small cohort NP programs: The recognition problem
Programs with smaller cohorts often foster close faculty relationships and supportive learning environments. But beneath that intimacy lies a structural challenge: limited program recognition creates compounding disadvantages that even the most dedicated faculty can't fully offset.
When program recognition shapes program capacity:
- Less visibility makes securing quality clinical placements harder to compete for
- Limited resources mean students navigate a fragmented mix of tools without unified support
- Faculty are stretched thin, filling gaps that better-resourced programs solve through infrastructure
As a result, student success becomes dependent on individual effort rather than systemic support.
The shared challenge across NP programs
Despite these structural differences, NP programs are ultimately trying to solve the same problem: How do you track an internal, evolving cognitive process using external, static tools?
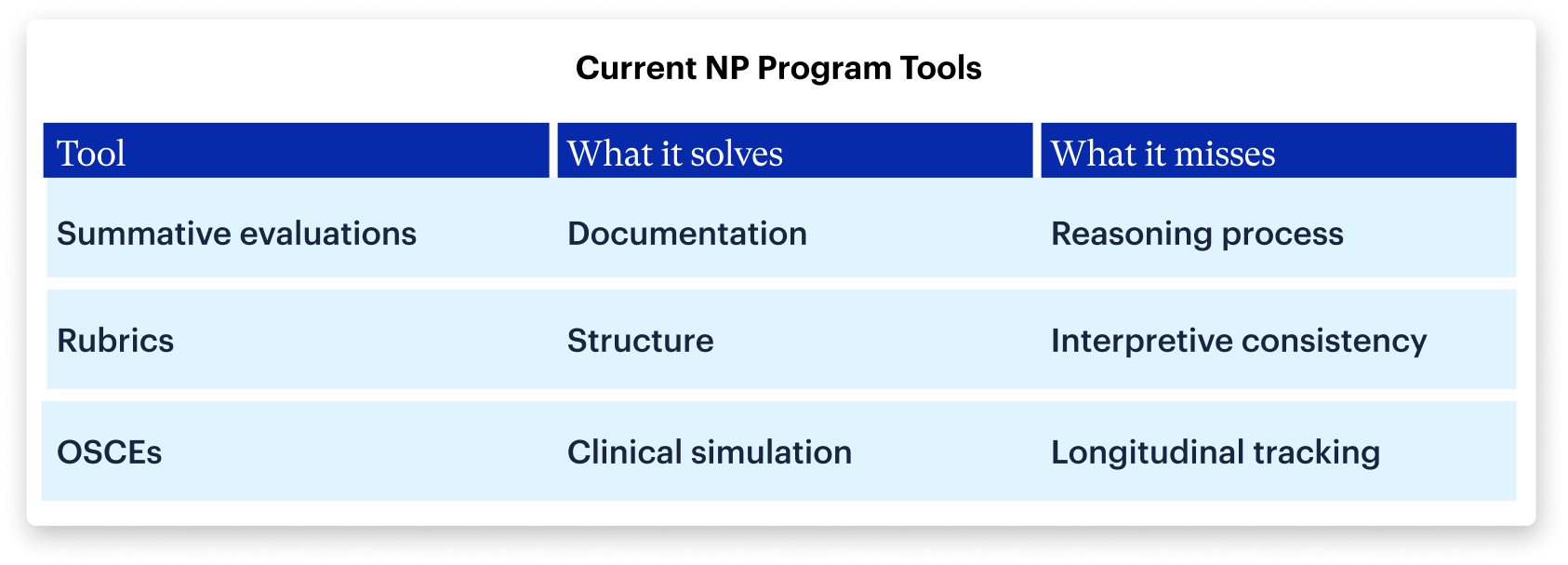
But none of these tools simultaneously provide:
- Direct visibility into clinical reasoning
- Consistent evaluation across sites
- Longitudinal tracking across training
What NP education lacks is shared infrastructure built to do two things: identify gaps in clinical reasoning early, and trigger remediation before those gaps follow a student into the clinical — all without piling more onto already-stretched faculty.
DDx by Sketchy: A new standard for clinical reasoning assessment in NP programs
DDx by Sketchy recreates the full arc of an NP patient encounter, from initial assessment and differential diagnosis through diagnostics, management decisions, and patient education. Built by clinicians, it gives faculty something they've rarely had: direct visibility into how students think.
Students move step-by-step through a clinical case, from initial patient presentation through history and physical exam findings, differential diagnosis generation, diagnostic testing decisions, treatment and management planning, and patient education. At each stage, the platform captures how the student is thinking, not just the final answer.
"[The students] are learning so much that even when the cases are challenging, they feel like they walk away with a better understanding of how to care for that patient."
— Bryanna Scherer, MSN, APRN, AGNP-C, OCN, Assistant Professor of Nursing at Missouri Baptist University
Faculty can see which diagnoses students initially consider, how they prioritize and narrow their differential, which clinical findings influence their reasoning, and where incorrect assumptions or premature closure occur. This provides something NP educators have historically lacked: direct visibility into clinical reasoning development.
88% of students at Hawaii Pacific University Psychiatric Mental Health Nurse Practitioner Program said they felt more prepared for OSCEs and clinical check-ins.
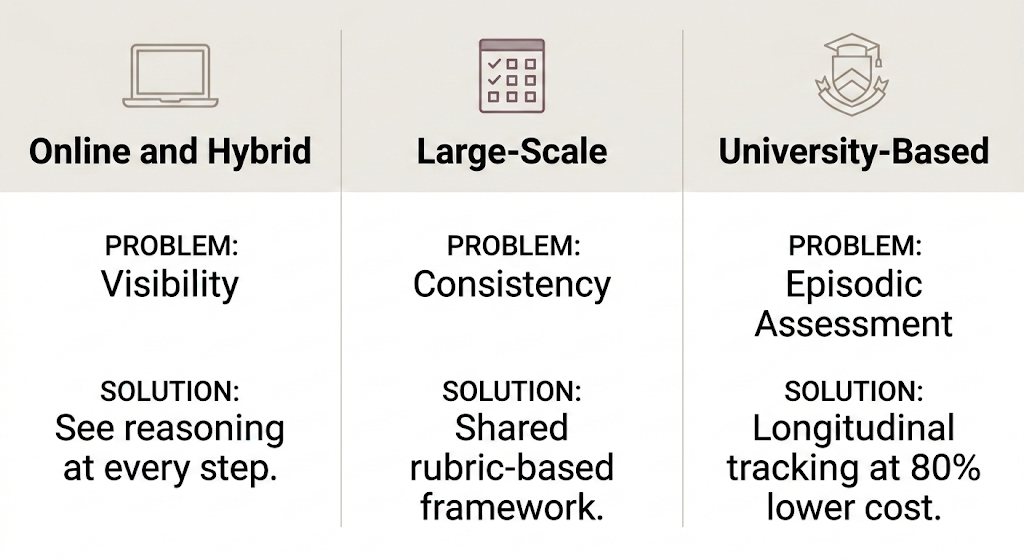
For online and hybrid programs
DDx provides direct visibility into student reasoning by showing how learners construct and narrow a differential diagnosis, where they hesitate or reconsider, and which diagnoses they prematurely rule out — allowing faculty to identify reasoning gaps early enough to intervene.
For large-scale programs
DDx introduces a shared, rubric-based framework applied consistently across learners regardless of clinical site or preceptor. Program leaders can monitor individual and cohort-level reasoning trends, generate defensible assessment data, and maintain consistent evaluation standards across distributed sites.
For smaller cohort programs
DDx directly addresses the structural barriers smaller programs face — giving programs the infrastructure and resource efficiency that were previously out of reach. With DDx, programs can build a rigorous, trackable record of student reasoning development, deploy cases at up to 80% lower cost than standardized patient OSCE equivalents, and cover all NP specialties without dependence on hard-to-secure clinical placements.
Designed to integrate across the NP curriculum
DDx cases can be scaffolded across all NP specialty tracks and training stages, including initial implementation in the 3 Ps (Pharmacology, Pathophysiology, Advanced Health Assessment) and continued implementation modularly in didactic courses and clinical practicums. Cases increase in complexity as students advance, helping programs align reasoning assessment with the progression of clinical training.
Frequently asked questions
Why is clinical reasoning so difficult to assess in NP programs?
Clinical reasoning is an internal cognitive process — faculty can observe what students do, but not how they think. Most evaluation tools measure outputs like written assignments or OSCE performance, which capture reasoning indirectly at best. The structural constraints of NP education — distributed clinical sites, variable preceptors, and limited direct observation — compound this challenge across all program types.
How do online NP programs assess clinical reasoning without direct observation?
Most online programs rely on written case submissions, clinical practicum reports, or periodic OSCEs — none of which give faculty real-time visibility into how students reason through a patient encounter. AI-powered simulation platforms address this gap by capturing every step a student takes in a case, making the reasoning process visible and comparable regardless of where or when the student is learning.
What is the cost difference between DDx and standardized patient OSCEs for NP programs?
Standardized patient OSCEs can cost upwards of $900 per student per assessment. DDx delivers OSCE-equivalent simulation at up to 80% lower cost, making large-scale, repeated assessment financially feasible for programs that currently limit OSCE frequency due to resource constraints.
When in the NP curriculum should clinical reasoning assessment begin?
Evidence supports introducing structured clinical reasoning assessment as early as the foundational coursework — the 3 Ps (Pharmacology, Pathophysiology, Advanced Health Assessment) — rather than waiting for clinical practicums. Early assessment allows programs to identify gaps when remediation is lower-stakes and more effective, before clinical responsibilities limit the time available for intervention.